MODULE #2
The immune system has two functions: defense and repair. If either the defense or repair function become overburdened or overstressed, immune dysfunction and disease may result. When important defense elements such as lymphocytes are mobilized against foreign antigens, the immune system can become overwhelmed and depleted. As a result, vital repair processes suffer and a state of inflammation ensues. Inflammation, rethought as “repair deficit,” is the result of prolonged unhealthy conditions that force the body to focus on defending rather than repairing.
Inflammation is often presented as a fire to be fought or a symptom to be suppressed. Chronic inflammation, or cumulative repair deficit, increases the probability of metabolic imbalance, weight management issues, and insulin resistance. This is reflected across the continuum between pre-diabetes, diabetes, and a myriad of consequences to the heart and blood vessels. Additionally, inflammation so imbalances immune responses that delayed allergies develop. Delayed or late-phase food reactions and other chemical sensitivities further contribute to chronic low-grade systemic inflammation and play a role in causing or amplifying autoimmune, chronic, and degenerative illnesses.
Types of Immune System Response.
 Classic allergy is the immediate IgE mediated immune response that triggers symptoms such as itchy eyes and runny nose, with symptoms starting almost immediately after exposure. Tests of immediate allergy measure IgE either by RAST blood tests or by in-office skin prick/scratch tests.
Classic allergy is the immediate IgE mediated immune response that triggers symptoms such as itchy eyes and runny nose, with symptoms starting almost immediately after exposure. Tests of immediate allergy measure IgE either by RAST blood tests or by in-office skin prick/scratch tests.
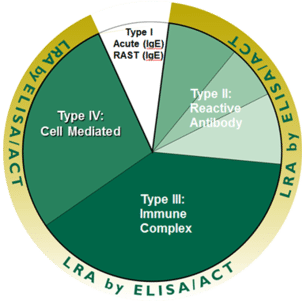
The delayed immune reactions, sometimes called delayed allergies, occur several hours to several weeks after exposure. There are three mechanisms for delayed hypersensitivity reactions:
- Reactive antibodies
- Immune complexes
- T Cell direct responses
The delay between exposure and noticeable symptoms makes identification of the offending substance virtually impossible through history alone. Functional tests are needed to accurately identify immune response-provoking substances, but all tests of hypersensitivity are not equal.
Tests of Hypersensitivity. What is Being Measured?
See LAB COMPARISON TABLE
The fundamental difference between the various hypersensitivity test methods lies in what is measured. There are tests that measure antibodies, tests that measure particle size or volume changes, and tests that directly measure live lymphocyte response.
Serology tests measure the physical presence and amount of an antibody or antibody sub-type. Examples of these tests include ELISA IgA, IgG, and IgG4 tests performed by labs such as Cyrex, Genova, MetaMetrix, and many others. Measurement of antibody reveals that at some time the immune system mounted a response. The same mechanism operates when we recover from infection and illness, and antibodies are formed.
Antibody tests such as IgG are imprecise because they are unable to distinguish between protective antibodies and those that are provoking reactions. As an example, consider someone who had chickenpox as a child and now has antibodies to chickenpox (although they do not currently have symptoms of the disease). The lack of differentiation between harmful and protective antibodies results in high rates of “false positive” reactions and ultimately makes it difficult for patients to comply with an avoidance program. Poor compliance, coupled with the fact other types of hypersensitivity (type III and type IV) are not detected with antibody tests, greatly limits the clinical outcomes seen with antibody tests such as IgG.
Other test methods measure markers, such as particle size or volume changes, which can be related to immune response. The weakness of these test methods is that immune response is not the only source of the markers being detected. For instance, in particle size testing, a machine is used to detect particles 10 microns or larger in size. The rationale for particle size as a marker of immune response is that reactive lymphocytes are 10 microns in size. However, reactive lymphocytes are not the only particles of that size. These devices have no way to distinguish reactive lymphocytes from platelet clumps, stacks of red cells, or granulocyte remnants, all which can be 10 microns or larger. A recent study by Hodsdon and Zwickey comparing two hypersensitivity test methods concluded that particle size testing has such poor reproducibility that results are essentially random and have no clinical value.
The Lymphocyte Response Assay (LRA) developed by Dr. Jaffe at ELISA/ACT Biotechnologies is the only test of delayed hypersensitivity that directly measures lymphocyte responses to the antigens being tested. By looking directly at the lymphocyte, rather than at some marker suggestive of an immune response, the LRA is uniquely able to identify the full range of delayed immune responses (reactive antibody, immune complex, and direct cell response).